STARTING FROM THE BEGGINING ~ ORIGIN OF THE AFRICAN PROBLEM
Sanitation is defined as the study and use of practical measures for the preservation of public health. These practical measures include sewage systems and clean water supplies that warrant places keeping on clean. As mentioned in previous posts, this means that the locations suffering from scarcity of water have to face an additional problem, which is the one related to the quality of that water. 2.3 billion of the world's population still do not have basic sanitation facilities, such as toilets or latrines; and more than 1.8 billion people are estimated to drink water that is not protected against contamination from faeces or other sanitary hazards (United Nations). In this post, I would like to adress the importance of sanitation and the role of civil engineering in the systems thought to provide it. I aim to analyse which are the main problems of water sanitation in Africa and the historical background that originated them. All this to finally post the question: which actions could be implemented in order to assess solutions?
As a continent, Africa is thought to have the lowest sanitation coverage in the world (J. Njoh, 2012), limited or lacking access to safe hygiene and sanitation facilities being the first cause of diarrhea, dysentery and typhoid, among other frequent diseases.

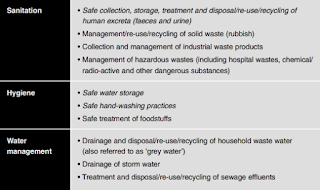
Figure 2. Image showing examples of some considered improved and unimproved sanitation systems (Global Water Supply and Sanitation Assessment, 2000).
Examples of the important (if not critical) contribution of urban planning (and from now on, let us understand urban planning as the principal tool of civil engineering in this context) in the solution or prevention of this problems would include the fight against malaria by ridding of human settlements of shubbery and standing water, in order to eliminate mosquito breeding grounds in the built environment; or the effective implementation of drainage systems and fitting openings of houses with screens (J. Njoh, 2012). Other actions taken in the field could also prevent health threats related to insalubrious conditions (caracterised by the indiscriminate disposal of waste, that boosts diseases such as dysentery, diarrhea, cholera and tuberculosis), traffic accidents (resulting from bad designed and maintained roads) and poverty.
Despite this evidences, urban planning has from its origin been split up from public health perspectives, arriving to the point that, although mortar drains and pipes and other basic drawning and distribution planning were common practices in ancient times, many hygiene and sanitation problems of the past are reocurring today (J. Njoh, 2012). This has been atributed to the fact that Egyptians, Mesopotamians, Hebrews ans Incas incourred in those sanitation measures upon the belief "cleanliness is next to godliness", that is, only for religious purposes. Instead of concioussness of the health reasons, the water and waste treatment infrastructures that were undertaken at that time were driven by the convincement that health problems were caused by supernatural forces, and therefore lacked of important environmental factors to further develop the measures.
It was not until the industralisation era that the sanitanitary reform movement (curious here do adress to HIST 234), born in England in the mid-1800, which finally brought illness to be regarded as originated by poor social and environmental conditions and not only morality and spirituality (C.S.F.P.H., 1988), promulgated the first sanitation an hygiene policies as we know them today, and it took until the European colonization in Africa to transplant the policies there. However, while in Europe efforts had been placed to providing the 'greatest good for the greatest numbers', implementation of the policies in Africa was focused on exclusively protecting the Europeans in the colonies, so minimal efforts were made for other districts (J. Njoh, 2012). One of the most important improvements driven by those policies were the building codes, which by regulating the construction of physical structures could assess sustainability, safety and other aspects related to public health. But just because Africa's contemporary codes are a legacy of what spreaded from the standards applied in European colonies, even nowadays their effectiveness and legitimacy is questionable (J. Njoh, 2012).
To heat up the issue, since the late-20th century, public health and town planning have notoriously drifted appart, mainly because germ theories arousen in the late-19th century drove health professionals to focus their energies in laboratory investigation rather than in the human physical environment. Even nowadays, most African countries have separated ministerial bodies for town planners and public health officials, and collaboration between them is rare (J. Njoh, 2012). This could be one of the causes for African countries not to meet the hygiene-and-sanitation-related targets of the Millenium Development Goals (if the reader is devoted to other blogs about the African problem, more detailed explanations of these goals can be found in sites such as Africa's Water Women, as well as the UN website).
Understanding of the origin on the sanitation problem in Africa cannot be taken as a mere historical study. It should aim to place an alarm at the fact that most of the past drawbacks are still in vogue. Indeed, this is worsen by the tend of some governments to still take the sanitation and hygiene issue as a taboo (Tearfund), which obstaculizes the implementation of correct policies and strategies. Some studies (Tearfund) have suggested that the steps to attaining the MDGs should include:
1. Assessing sanitation as a priority ~not only fighting against that taboo surrounding governmental attitudes, but also promoting the voices of women (the ones principally affected by poor water sanitation systems) to be heard.
2. Links with other sectors ~this means understanding that sanitation measures also affect, and are affected by, sectors such as education or health services.
3. Capacity ~in the sense of more funding, being implemented in big and small authorities and contruction responsibles.
4. Behaviour change ~this point is especially important, as community mobilisation and education is key to really attain public health in all aspects (here a personal annecdote: my mum, as a doctor, used to point out that no matter if you have a brush and a bar of toothpaste, if you do not know how to precisely brush your teeth, they will remain not clean. It is a matter of education in the sense of knowing how to use the resources, rather than just having them). Actually, education tends to drive a way greater impact than the simple application of measures such as construction of latrines.
In relation to this last reflection, any technology or science innovations are a product of the human intelligence and commitment, and therefore the only way to hope for a real change is to hang on and spread the knowledge as far as it is possible. As suggested already several times in this blog, evolution is not only a long-term feat, but also something that we all have to accomplish together.

Comments
Post a Comment
Let me know what you think about this!